Definition
Histoplasmosis is an infectious disease caused by inhaling the microscopic spores of the fungus Histoplasma capsulatum.
The disease exists in three forms. Acute or primary histoplasmosis
causes flulike symptoms. Most people who are infected recover without
medical intervention. Chronic histoplasmosis affects the lungs and can
be fatal. Disseminated histoplasmosis affects many organ systems in the
body and is often fatal, especially to people with acquired immunodeficiency syndrome (AIDS).
Description
 Histoplasmosis
is an airborne infection. The spores that cause this disease are found
in soil that has been contaminated with bird or bat droppings. In the
United States, the disease is most common in eastern and midwestern
states and is widespread in the upper Mississippi, Ohio, Missouri, and
St. Lawrence river valleys. Sometimes histoplasmosis is called Ohio
Valley disease, Central Mississippi River Valley disease, Appalachian
Mountain disease, Darling's disease, or Histoplasma capsulatum infection.
Histoplasmosis
is an airborne infection. The spores that cause this disease are found
in soil that has been contaminated with bird or bat droppings. In the
United States, the disease is most common in eastern and midwestern
states and is widespread in the upper Mississippi, Ohio, Missouri, and
St. Lawrence river valleys. Sometimes histoplasmosis is called Ohio
Valley disease, Central Mississippi River Valley disease, Appalachian
Mountain disease, Darling's disease, or Histoplasma capsulatum infection.
Anyone
can get histoplasmosis, but people who come in contact with bird and
bat excrement are more likely to be infected. This includes farmers,
gardeners, bridge inspectors and painters, roofers, chimney cleaners,
demolition and construction workers, people installing or servicing
heating and air conditioning units, people restoring old or abandoned
buildings, and people who explore caves.
The
very young and the elderly, especially if they have a pre-existing lung
disease or are heavy smokers, are more likely to develop symptoms that
are more severe. People who have a weakened immune system, either from
diseases such as AIDS or leukemia, or as the result of medications they
take (corticosteroids, chemotherapy drugs), are more likely to develop chronic or disseminated histoplasmosis.
Causes and symptoms
When the spores of H. capsulatum
are inhaled, they lodge in the lungs where they divide and cause
lesions. This is known as acute or primary histoplasmosis. It is not
contagious.
Many otherwise healthy people show
no symptoms of infection at all. When symptoms do occur, they appear
3-17 days after exposure (average time is 10 days). The symptoms are
usually mild and resemble those of a cold or flu; fever,
dry cough, enlarged lymph glands, tiredness, and a general feeling of
ill health. A small number of people develop bronchopneumonia. About 95%
of people who are infected either experience no symptoms or have
symptoms that clear up spontaneously. These people then have partial
immunity to re-infection.
In some people, the
spores that cause the disease continue to live in the lungs. In about 5%
of people who are infected, usually those with chronic lung disease,
diabetes mellitis, or weakened immune systems, the disease progresses to
chronic histoplasmosis. This can take months or years. Symptoms of
chronic histoplasmosis resemble those of tuberculosis.
Cavities form in the lung tissue, parts of the lung may collapse, and
the lungs fill with fluid. Chronic histoplasmosis is a serious disease
that can result in death.
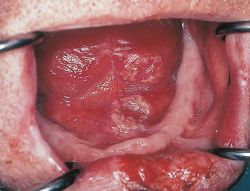
The rarest form of
histoplasmosis is disseminated histoplasmosis. Disseminated
histoplasmosis is seen almost exclusively in patients with AIDS or other
immune defects. In disseminated histoplasmosis the infection may move
to the spleen, liver, bone marrow, or adrenal glands. Symptoms include a
worsening of those found in chronic histoplasmosis, as well as weight
loss, diarrhea, the development of open sores in the mouth and nose, and enlargement of the spleen, liver, and adrenal gland.
Diagnosis
A simple skin test similar to that given for tuberculosis will tell if a person has previously been infected by the fungus H. capsulatum.
Chest x rays often show lung damage caused by the fungus, but do not
lead to a definitive diagnosis because the damage caused by other
diseases has a similar appearance on the x ray. Diagnosis of chronic or
disseminated histoplasmosis can be made by culturing a sample of sputum
or other body fluids in the laboratory to isolate the fungus. The urine,
blood serum, washings from the lungs, or cerebrospinal fluid can all be
tested for the presence of an antigen produced in response to the
infection. Most cases of primary histoplasmosis go undiagnosed.
Treatment
Acute primary histoplasmosis generally requires no treatment other than rest. Non-prescription drugs such as acetaminophen (Tylenol) may be used to treat pain and relieve fever. Avoiding smoke and using a cool air humidifier may ease chest pain.
Patients
with an intact immune system who develop chronic histoplasmosis are
treated with the drug ketoconazole (Nizoral) or amphotericin B
(Fungizone). Patients with suppressed immune systems are treated with
amphotericin B, which is given intravenously. Because of its potentially
toxic side effects, hospitalization is often required. The patient may
also receive other drugs to minimize the side effects of the
amphotericin B.
Patients with AIDS must
continue to take the drug itraconazole (Sporonox) orally for the rest of
their lives in order to prevent a relapse. If the patient can not
tolerate itraconazole, the drug fluconazole (Diflucan) can be
substituted.
Alternative treatment
In
non-immunocompromised patients, alternative therapies can be very
successful. Alternative treatment for fungal infections focuses on
creating an environment where the fungus cannot survive. This is
accomplished by maintaining good health and eating a diet low in dairy
products, sugars, including honey and fruit juice, and foods like beer
that contain yeast. This is complemented by a diet high in raw food.
Supplements of antioxidant vitamins C, E, and A, along with B complex, may also be added to the diet. Lactobacillus acidophilus and Bifidobacteria
will replenish the good bacteria in the intestines. Antifungal herbs,
like garlic, can be consumed in relatively large does and for an
extended period of time in order to be most effective.
Prognosis
Most
people recover from primary histoplasmosis in a few weeks without
medical intervention. Patients with chronic histoplasmosis who are
treated with antifungal drugs generally recover rapidly if they do not
have an underlying serious disease. When left untreated, or if serious
disease is present, histoplasmosis can be fatal.
AIDS
patients with disseminated histoplasmosis vary in their response to
amphotericin B, depending on their general health and how well they
tolerate the side effects of the drug. Treatment often suppresses the
infection temporarily, but patients with AIDS are always in danger of a
relapse and must continue to take medication for the rest of their lives
to keep the infection at bay. New combinations of therapies and new
drugs are constantly being evaluated, making hard statistics on
prognosis difficult to come by. AIDS patients have problems with
multiple opportunistic infections, making it difficult to isolate death rates due to any one particular fungal infection.
Prevention
Since the spores of H. capsulatum
are so widespread, it is almost impossible to prevent exposure in
endemic areas. Dust suppression measures when working with contaminated
soil may help limit exposure. Individuals who are at risk of developing
the more severe forms of the disease should avoid situations where they
will be exposed to bat and bird droppings.
Key terms
Acidophilus — The bacteria Lactobacillus acidophilus, usually found in yogurt.
Adrenal gland
— A pair of organs located above the kidneys. The outer tissue of the
gland produces the hormones epinephrine (adrenaline) and norepinephrine,
while the inner tissue produces several steroid hormones.
Antigen — A foreign protein to which the body reacts by making antibodies.
Bifidobacteria — A group of bacteria normally present in the intestine. Commercial supplements are available.
Corticosteroids
— A group of hormones produced naturally by the adrenal gland or
manufactured synthetically. They are often used to treat inflammation.
Examples include cortisone and prednisone.
Resources
Organizations
American Lung Association. 1740 Broadway, New York, NY 10019. (800) 586-4872. http://www.lungusa.org.
Histoplasmosis: Protecting Workers at Risk. Centers for Disease Control and Prevention. http://www.cdc.gov/niosh/97146eng.html.
No comments:
Post a Comment